The complexity and challenges of delivering health service supports relies on an equally robust, efficient, and effective medical command and control structure.
War is a human endeavor, fought and won by soldiers whose overall health and fighting spirit are fundamental to the outcomes of war. The military owes its soldiers and the joint force commanders who lead them the capability and capacity to optimize collective health and fighting spirit before, during, and after conflict. Bridging the joint functions of sustainment and protection, robust health service support maintains, sustains, protects, and conserves the collective soldier physical health and mental well-being necessary to win on the modern battlefield. The complexity and challenges of delivering health service supports relies on an equally robust, efficient, and effective medical command and control structure. Logically, one would assume command and control of medical resources would be highly prioritized, organized, and integrated with similar frameworks in combined arms and other support functions. This is not the case. While emphasis on and prioritization of combined arms ensures command and control doctrine and resourcing in those areas are continually scrutinized, the concept and resourcing of command and control in health service support remains atrophied and poorly integrated into the combined arms functions it supports. The critical role medical support plays in generating, sustaining, and conserving one of the joint force commander’s most important assets—people—demands some attention and efforts to better integrate, synchronize, and nest it within the larger context of joint command.
Great power competition and conflict loom large in defense planning and programs. With great power competition comes the potential for conflicts of a scale and tempo not experienced in the contemporary era. This environment will create tremendous amounts of data and success on any future battlefield may depend upon skill and efficiency in sorting through this data to make connections between information points from myriad sources to inform decision-making. In essence, command—decision-making as it relates to identifying objectives, allocating resources, and accepting risks—and control—the elements required to carry out command decisions—rely on data and how we manage it to create information. Future conflict spaces will offer lots of data. The integration, connection, and interpretation of actively and passively collected data from multiple sources must converge to paint the landscape informing a commander’s judgement. The projected tempo of future conflict requires near-instantaneous alteration of this landscape to inform decisions that must happen in seconds, minutes, or hours.
Realizing the imperative of data management in the battle space and current limitations to data integration, modernization of command and control systems is a priority of the National Defense Strategy. Joint All-Domain Command and Control (JADC2) is the proposed solution. The JADC2 concept combines intelligence, surveillance, and reconnaissance data transmitted across communication networks from all services and converges them into a single system, ultimately connecting sensors to shooters. Artificial intelligence and automation integration into JADC2 holds potential to augment expeditious data sifting and interpretation in support of decision making. The aim is to collect, converge, connect, and sort data to produce the information required to support command and control in a data-saturated and lethal environment. JADC2 may go a long way in bringing together data from disparate systems across the services but it also holds potential to bridge command and control between support and combat arms elements. Specifically, JADC2 could help to standardize medical command and control and link it to the combat elements it exists to support.
Stewarding limited capabilities and capacity over time is a primary element of command and critical to the high demand resourcing inherent to great power conflict. People are a limited resource and medical support is a prime enabler of their maintenance, but its capacity is limited. Medical capacity may be one of the greatest challenges of great power conflict. The conflicts in Afghanistan and Iraq did not fully test joint force medical capacity; annual casualty numbers never exceeded the one day casualty numbers from D-day. Medical capacity limitations impact operational timing, tempo, and scale considerations. Capabilities are also limited and may require deliberate planning tradeoffs. Medical functions generally benefit from economies of scale, so sacrificing capability and capacity to facilitate wider dispersion and proximity of health support provides an example; additionally, the availability of evacuation corridors could dictate the timing and feasibility of operations. The command function of resource allocation relies upon convergence of medical data to inform planning at all levels.
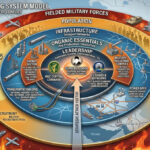
Globally Integrated Health Services (GIHS) is the Joint Force concept for synchronization and strategic management of joint operational health services. GIHS aims to support Joint Force Commanders by quickly synchronizing and combining medical capabilities that are networked, modular, and interoperable, providing tailored support to meet specific operational and strategic requirements. Seven core ideas describe GIHS:
- Integrated joint requirements in medical force development
- Global synchronization of health services
- Modular and interoperable medical capabilities
- Global networking of health service nodes
- Tailored medical forces and operations
- Leader integration into joint medical capabilities to synchronize multiple efforts across multiple domains to ensure unity of health service efforts
- Improved performance
From the standpoint of medical command and control across the joint force, a current problem is there is no standardized way or means of reporting command and control-essential data and information related to health service support.
What the GIHS concept currently lacks is an imperative to impose a standardized, consolidated collection and reporting tool that can communicate data relevant to the core ideas across domains and present a true picture of the decision-making landscape, informed by health support factors and their interaction within and between other domains, for medical commanders and the Joint Force Commanders they support.
From the standpoint of medical command and control across the joint force, a current problem is there is no standardized way or means of reporting command and control-essential data and information related to health service support. What are the data points to indicate if there is unity of health service efforts across multiple domains? How do we measure and report performance? How do we tailor medical forces to specific operations? How is this information communicated or available to medical commanders and all levels of command they support? From the non-medical commander’s perspective, a current problem is there is no standardized way or means by which health service support data and information is fed into the data pool to mix with data from other domains so that connections, linkages, and dependencies are identified. The result is that commanders may be largely blind to medical constraints or opportunities that should inform resource allocation, risk assessment, and operational objectives.
The JADC2 concept provides an opportunity to shore up these gaps if its design is deliberate in incorporating health service intelligence, surveillance, and reconnaissance. This would require recognition of the current challenges to medical command and control and the indelible contribution of health service support to combat power. Fundamentally, medical injects into JADC2 should reflect standardized medical functions, as exemplified by the Army’s 10 warfighting medical functions:
- Medical command and control
- Medical treatment (organic and area support)
- Hospitalization
- Medical evacuation (to include medical regulating)
- Dental services
- Operational public health
- Combat and operational stress control
- Veterinary services
- Medical logistics (to include blood management)
- Medical laboratory services (to include both clinical laboratories and environmental laboratories)
These functions are dovetailed with the seven core ideas of GIHS and the automation and artificial intelligence potential in the JADC2 concept could integrate and describe these linkages with other data points in the environment while accelerating health service data processing, information generation, and decision making. As an example of how JADC2 could link the medical functions with GIHS and across the multi-domain battle space to inform command and control, consider the medical evacuation function and the GIHS idea of globally networked health service nodes. When an injury occurs and evacuation is indicated, data about the injury is created—the type of injury, likely medical intervention required, location and environmental context of the injury. This data could be linked with other data points fed into JADC2 to determine the most appropriate means for evacuation, the route for evacuation and the medical facility most aligned with the capabilities to treat the injury while accounting for constraints of the environment. For instance, the closest medical facility may be low on blood or overwhelmed with other injuries; integrated data could identify a treatment facility at further distance with improved capacity and capability to care for the injury. When a capability is unavailable, multiple injuries threaten to saturate capacity or create potential impose culmination constraints or if collected data suggest a pattern of injury indicative of a previously unrecognized threat (such as chemical weapons), data integration, convergence and interpretation using automation and artificial intelligence as JADC2 may be designed to do, could provide an early warning sign and signal decision points for commanders. JADC2 holds tremendous potential to fill a substantial gap in medical command and control and better network health service support to the myriad other networks existing at all levels of battle. To do this, however, we need to think beyond domains and look to all the major networks of data that need to be linked to allow commanders to command and control. Air, land, sea, space, and cyber may be the domains capturing our current attention but there are background elements that paint the landscapes of which these domains are the focus. The challenge of our current “domain” conception may be that those domains fail to encompass all the elements and systems at work within a battle space. It’s a useful conception if we realize there are factors and systems at work outside the air, land, sea, space, and cyber domains and think beyond these conventions. Planning should account for as many variables and networks at play in the environment as possible and medical (along with the sustainment function within which it is nested) is big one and one that should not be overlooked when modernizing tools for command and control. The background and the foreground create the landscape and every aspect of the image is dependent on the others to create the fullest impression.
Alison Batig is a Colonel and physician/surgeon in the U.S. Army. She is a member of the AY22 Resident Class of the U.S. Army War College.
The views expressed in this article are those of the author and do not necessarily reflect those of the U.S. Army War College, the U.S. Army, or the Department of Defense.
Photo Description: Low light surgery as conducted by Special Operations Surgical Team. Commonly referred to as SOST’s, they are teams of lightweight, mobile surgical specialists with advanced medical and tactical training to save lives, anywhere and anytime.
Photo Credit: Photo by SrA Keith James, courtesy of Air Force Special Tactics (24 SOW) homepage